
The US has experienced more deaths from coronavirus disease 2019 (COVID-19) than any other country and has one of the highest cumulative per capita death rates.1,2 An unanswered question is to what extent high US mortality was driven by the early surge of cases prior to improvements in prevention and patient management vs a poor longer-term response.3 We compared US COVID-19 deaths and excess all-cause mortality in 2020 (vs 2015-2019) to that of 18 countries with diverse COVID-19 responses.
Methods
We compared the US with Organisation for Economic Co-operation and Development countries with populations exceeding 5 million and greater than $25 000 per capita gross domestic product. For each country, we calculated the COVID-19 per capita mortality rate and grouped countries by mortality: (1) low (COVID-19 deaths, <5/100 000), (2) moderate (5-25/100 000), and (3) high (>25/100 000).1 We used Poisson regression for comparisons across countries.
We calculated the difference in COVID-19 deaths between each country and the US through September 19, 2020 (week 38) under 3 scenarios: if the US had a comparable per capita COVID-19 mortality rate to each country from the start of the pandemic (February 13) or if the US mortality rate became comparable to other countries beginning May 10 or June 7, to allow lag time for policy interventions.3 (See the Supplement for formulas.)
Results
On September 19, 2020, the US reported a total of 198 589 COVID-19 deaths (60.3/100 000), higher than countries with low and moderate COVID-19 mortality but comparable with high-mortality countries (Table 1). For instance, Australia (low mortality) had 3.3 deaths per 100 000 and Canada (moderate mortality) had 24.6 per 100 000. Conversely, Italy had 59.1 COVID-19 deaths per 100 000; Belgium had 86.8 per 100 000. If the US death rates were comparable to Australia, the US would have had 187 661 fewer COVID-19 deaths (94% of reported deaths), and if comparable with Canada, 117 622 fewer deaths (59%).
While the US had a lower COVID-19 mortality rate than high-mortality countries during the early spring, after May 10, all 6 high-mortality countries had fewer deaths per 100 000 than the US. For instance, between May 10 and September 19, 2020, Italy’s death rate was 9.1/100 000 while the US’s rate was 36.9/100 000. If the US had comparable death rates with most high-mortality countries beginning May 10, it would have had 44 210 to 104 177 fewer deaths (22%-52%) (Table 1). If the US had comparable death rates beginning June 7, it would have had 28% to 43% fewer reported deaths (as a percentage overall).
In the 14 countries with all-cause mortality data, the patterns found for COVID-19–specific deaths were similar for excess all-cause mortality (Table 2). In countries with moderate COVID-19 mortality, excess all-cause mortality remained negligible throughout the pandemic. In countries with high COVID-19 mortality, excess all-cause mortality reached as high as 102.1/100 000 in Spain, while in the US it was 71.6/100 000. However, since May 10 and June 7, excess all-cause mortality was higher in the US than in all high-mortality countries (Table 2).

Discussion
Compared with other countries, the US experienced high COVID-19–associated mortality and excess all-cause mortality into September 2020. After the first peak in early spring, US death rates from COVID-19 and from all causes remained higher than even countries with high COVID-19 mortality. This may have been a result of several factors, including weak public health infrastructure and a decentralized, inconsistent US response to the pandemic.4,5
Limitations of this analysis include differences in mortality risk: the US population is younger but has more comorbidities compared with the other countries.6 In addition, since late August death rates have increased in several countries, and how mortality will compare with the US throughout fall remains unknown.
Article Information
Accepted for Publication: October 2, 2020.
Published Online: October 12, 2020. doi:10.1001/jama.2020.20717
Concept and design; acquisition, analysis, or interpretation of data; and drafting of the manuscript: Both authors.
Critical revision of the manuscript for important intellectual content: Emanuel.
Statistical analysis: Bilinski.
Obtained funding: Emanuel.
Administrative, technical, or material support: Emanuel.
Supervision: Emanuel.
Conflict of Interest Disclosures: Dr Emanuel reported receiving personal fees and nonfinancial support from Blue Cross Blue Shield Minnesota, Bergen University, United Health Group, Futures Without Violence, Children’s Hospital of Philadelphia, Washington State Hospital Association, the Association of Academic Health Centers, Blue Cross Blue Shield of Massachusetts, Lumeris, Roivant Sciences, Medical Specialties Distributors, Vizient University Health System Consortium, the Center for Neurodegenerative Disease Research, Genentech Oncology, the Council of Insurance Agents and Brokers, America’s Health Insurance Plans, the Montefiore Physician Leadership Academy, Medical Home Network, the Healthcare Financial Management Association, Ecumenical Center–UT Health, the American Academy of Optometry, the Associação Nacional de Hospitais Privados, the National Alliance of Healthcare Purchaser Coalitions, Optum Labs, the Massachusetts Association of Health Plans, the District of Columbia Hospital Association, Washington University, Optum, Brown University, McKay Lab, the American Society for Surgery of the Hand, the Association of American Medical Colleges, America’s Essential Hospitals, Johns Hopkins University, the National Resident Matching Program, Shore Memorial Health System, Tulane University, Oregon Health and Science University, Blue Cross Blue Shield, and the Center for Global Development, as well as nonfinancial support from the Delaware Healthcare Spending Benchmark Summit, Geisinger Health System, RAND Corporation, Goldman Sachs, The Atlantic, Village MD, and Oncology Analytics. Dr Emanuel is also a venture partner at Oak HC/FT, and a partner at Embedded Healthcare LLC and COVID-19 Recovery Consulting. Ms Bilinski reported no disclosures.
Funding/Support: This research was partially funded by the Colton Foundation.
Role of the Funder/Sponsor: The Colton Foundation had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Additional Contributions: We thank David Cutler, PhD, of the Harvard University Department of Economics, for helpful feedback, for which he received no compensation.
Additional Information: Data and code are publicly available on GitHub.



David Icke: There is No Virus– The Latest Proof
https://banned.video/watch?id=5fc4fb577d10ea55e779a448
(Somebody please send this to Donald Trump)
The article by Ezekiel is not the correct one in this context. The Johns Hopkins study was authored by Dr. Briand and showed no excess deaths overall in the U.S. this year. Ezekiel is the brother of Rahm Emanuel and has been tapped by Biden (if he is ever truly elected) to head the COVID task force. He and his brother are members of the ruling cabal and his article shows excess deaths overall due to COVID, which is a bogus finding.
Great catch, William. A colleague observed that, in several countries, CV made no difference to mortality, which of course should not be the case if it’s actually a causal factor affecting death. But that he is the brother of Rahm Emanuel is striking.
I would trust John Hopkins above anything from JAMA, which would simply represent the ‘official” narrative re the ‘vid. But, even if you take the JAMA article on face value, where’s the detail that explains exactly what a ‘vid-19 death means….? Well, it can only mean one thing when taken in context since the virus has never been isolated (and for me, does not even exist as such)….someone died WITH a cold virus in their system…..not FROM the virus. If I missed the detail that explains otherwise, will someone please point it out.
Quite simply, what all this means is that numbers and statistics have been manipulated to attribute deaths to the ‘vid….. supported by the fact that overall deaths world wide and US wide have not increased.
This is irrefutable.
Game over.
Psyop over.
Rappoport’s excellent report in regard to the John Hopkin’s article…
by Jon Rappoport
“This patient who died had an ordinary heart attack.”
“Not anymore. We’re repackaging it as COVID.”
by Jon Rappoport
November 30, 2020
Don’t blink. Johns Hopkins may delete or retract their analysis at any moment. Their author’s study is devastating. Too hot to handle.
UPDATE: Yes, I wrote that opener a few hours before Johns Hopkins stepped in and DID retract the article. Boom. [1] [2] [3] [4]
Hopkins claims the article has been used to spread misinformation about the pandemic, and contains factual errors. CDC is cited as one correct source of facts. Hmm.
Regardless, here is my article, finished before the Johns Hopkins retraction. Since then, I’ve only polished it a bit in several places, for clarity:
Months ago, I told you this, in a number of articles: The overwhelming percentage of people who are “dying from the virus” are actually dying from traditional diseases.
These people have been relabeled and repackaged as “COVID-19.”
It has nothing to do with “the virus.”
A new analysis from Johns Hopkins confirms this in spades.
The Johns Hopkins News-Letter article, in a student publication, is headlined, “A closer look at US deaths due to COVID-19.” It lays out the case made by “Genevieve Briand, assistant program director of the Applied Economics master’s degree program at Hopkins.”
As you keep reading, keep this in mind: If the so-called increase in mortality from COVID is offset, almost exactly, by a decrease in deaths from all other major diseases…
Indicating that the so-called COVID deaths are nothing more than an exercise in re-labeling, then…
You can say there is a new coronavirus, but it’s even less harmful than flu, because virtually everybody recovers…
Or you can say the whole story of a new coronavirus is a fake narrative. There is no new virus.
My readers know I’ve been offering much evidence for the latter conclusion.
Here are key quotes from the Johns Hopkins News-Letter article:
“These data analyses suggest that in contrast to most people’s assumptions, the number of deaths by COVID-19 is not alarming. In fact, it has relatively no effect on deaths in the United States.”
“This comes as a shock to many people. How is it that the data lie so far from our perception?”
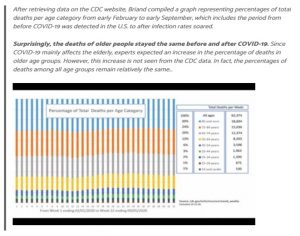
“When Briand looked at the 2020 data during that seasonal period, COVID-19-related deaths exceeded deaths from heart diseases. This was highly unusual since heart disease has always prevailed as the leading cause of deaths. However, when taking a closer look at the death numbers, she noted something strange. As Briand compared the number of deaths per cause during that period in 2020 to [deaths per cause in] 2018, she noticed that instead of the expected drastic increase across all causes, there was a significant decrease in deaths due to heart disease. Even more surprising, as seen in the graph below, this sudden decline in deaths is observed for all other causes.”
“This trend is completely contrary to the pattern observed in all previous years. Interestingly, as depicted in the table below, the total decrease in deaths by other causes almost exactly equals the increase in deaths by COVID-19. This suggests, according to Briand, that the COVID-19 death toll is misleading. Briand believes that deaths due to heart diseases, respiratory diseases, influenza and pneumonia may instead be [may have been] recategorized as being due to COVID-19.”
“The CDC classified all deaths that are related to COVID-19 simply as COVID-19 deaths. Even patients dying from other underlying diseases but are infected with COVID-19 count as COVID-19 deaths. This is likely the main explanation as to why COVID-19 deaths drastically increased while deaths by all other diseases experienced a significant decrease.”
“’All of this points to no evidence that COVID-19 created any excess deaths. Total death numbers are not above normal death numbers. We found no evidence to the contrary,’ Briand concluded.”
“’If [the COVID-19 death toll] was not misleading at all, what we should have observed is an increased number of heart attacks and increased COVID-19 numbers. But a decreased number of heart attacks and all the other death causes doesn’t give us a choice but to point to some misclassification [re-labeling],’ Briand replied.”
“In other words, the effect of COVID-19 on deaths in the U.S. is considered problematic only when it increases the total number of deaths or the true death burden by a significant amount in addition to the expected deaths by other causes. Since the crude number of total deaths by all causes before and after COVID-19 [was first announced] has stayed the same, one can hardly say, in Briand’s view, that COVID-19 deaths are concerning.”
Of course, there is some mealy-mouthed backtracking in the article. The virus is deadly and the pandemic is real, etc. But the data are the data.
The whole COVID operation is a hoax.
If I thought other honest researchers would investigate and re-calculate the Hopkins analysis, I would say, let’s see what they come up with. But based on my experience, there will be, at best, a brief flurry of articles in the press about this extraordinary finding, and then the scientific and press denizens will move on, as if nothing happened. That is their way. They briefly expose a scandal and then they slither off to cover up the scandal.
The other possibility is: Hopkins will retract the analysis, claiming it was flawed. That is the other strategy the low-crawling creatures sometimes deploy.
So there you have it.
Hoax. Con. Fake.
As I keep reporting, the virus (never proven to exist) is the cover story for the true phase-one goal: destruction of the economy.
If the virus were real, if it were attacking people left and right, the all-cause mortality numbers would be through the roof.
But they aren’t.
“I have a great idea, Bill. Let’s declare a fake pandemic. We’ll report all sorts of high death numbers. But really, we’ll just be subtracting numbers from other traditional diseases that cause deaths, and we’ll add those numbers to our fake pandemic.”
“Sounds great, Tony. Can you pull it off? I mean, it’s pretty obvious.”
“Sure, we can pull it off. And if some journalist with a mainstream reputation or an institution suddenly develops a brief infection of ETHICS, we’ll call their work a mistake or a lapse in judgment.”
“You mean an institution like the World Health Organization or Johns Hopkins?”
“Right. We’ll say the institution didn’t issue the study, it was just one of their people, a lone researcher. And if necessary, the institution, under pressure, will back off. But that’s assuming anyone noticed the study in the first place. Normally, these ‘revelations’ surface for a moment and then sink like a stone. No one cares. A pandemic is a money waterfall. The beneficiaries won’t sacrifice their bottom lines, or their reputations…”
Of course, people can rise up and raise holy hell.
JAMA is part of the medical wing of the Bilderberger/Trilateralist/Deep State. The medical wing is accompanied by the financial wing, the intelligence wing, the law enforcement wing, the entertainment wing, the educational wing, the political wing, the “pseudo-scientific” wing, etc.
Nearly 20 years ago, JAMA published an article supporting the “lone gunman” JFK theory, upon which Dr. Cyril Wecht (the famous coroner and anti-Warren Commission medical authority) stated that JAMA “was now officially part of the government conspiracy”.
The tentacles of the cabal are many and large. They have been infiltrating all elements of American society for over a half-century, but a true patriot like Donald Trump–with the support of every other true patriot in America–will hopefully defeat them once and for all!
Maybe somebody should send this article to Donald Trump.
He thinks we all need a vaccine.